ECG Course
The ECG course consists of modules on Normal ECG, Atrial Fibrillation, Atrial Flutter, & SVT.
Please Login or register to view the course.ECG Course
 Introductory content here....
Introductory content here....
This course is available as a downloadable PDF or PowerPoint file and please download them using the following links:
Once you've had a chance to read through the course please return to this page and take the test.
ECG stands for Electrocardiogram
An ECG records the hearts electrical impulses and dictates this on a moving strip of paper, i.e. it shows the heart's electrical activity as line tracings. This can then be used to interpret the functioning of the heart and lead to an important diagnosis such as myocardial infarction, ventricular tachycardia, atrial fibrilation and subsequent management can then be started, hence is vitally important to be able to know and interpret ECG's.
This is a normal ECG wave form

This is a normal ECG seen on a rhythm strip
The componenets of the ECG - Basics
P wave : correlates to the right and left atrial depolarization
QRS Complex: The QRS represents the simultaneous activation of the right and left ventricles, (although most of the QRS waveform is associated with left ventricular depolarisation as in majority of cases the left ventricle of the heart is larger in comparison to the right)
ST segment: represents the isoelectric period when the ventricles are in-between depolarization and repolarization
T wave: represents the repolarization of the ventricles
Standard ECG settings
Frequency Response
0.05Hz – 150Hz (companies often set these at 0.5 Hz – 50HZ)
These are filtered ECGs and can alter isoelectric line placement & morphologies
- Gain sensitivity – calibration accuracy
- 5, 10, 20mm/mV (standard 10mm/mV)
Chart paper speed
- 25mm.sec– standard
- 50mm/sec
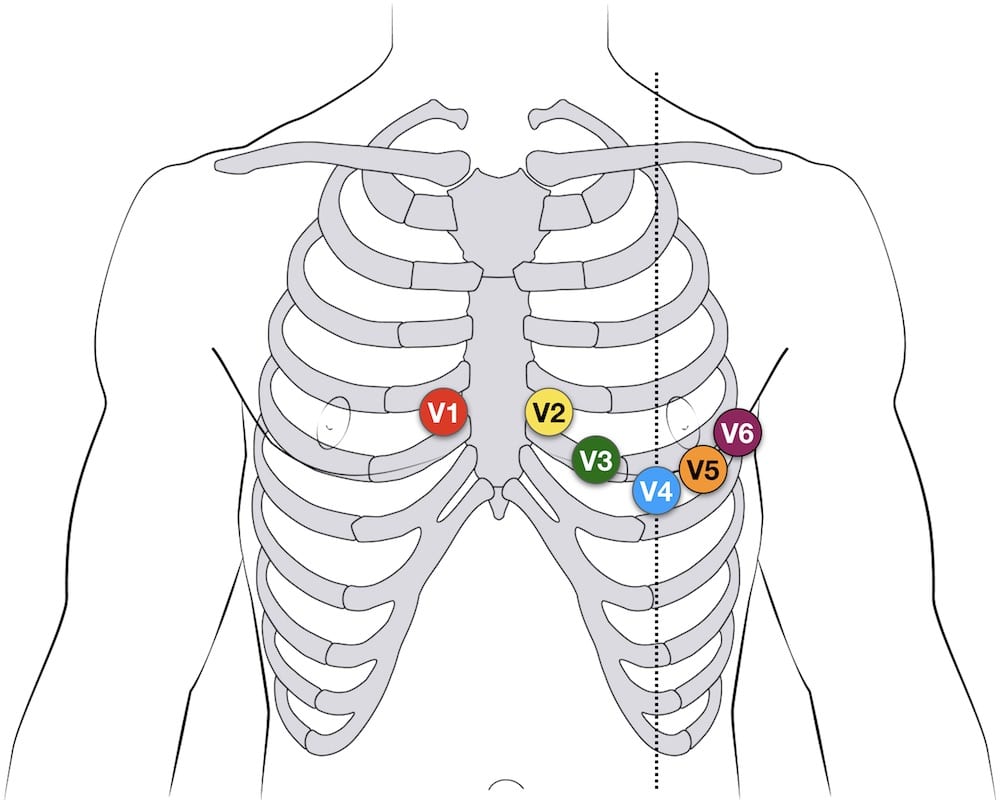
ECG Chest lead placement
•V1- 4thintercostal space at right sternal edge
•V2 – 4thintercostal space left sternal edge (not always dead opposite V1)
•V3 – midway diagonally between V2 & V4
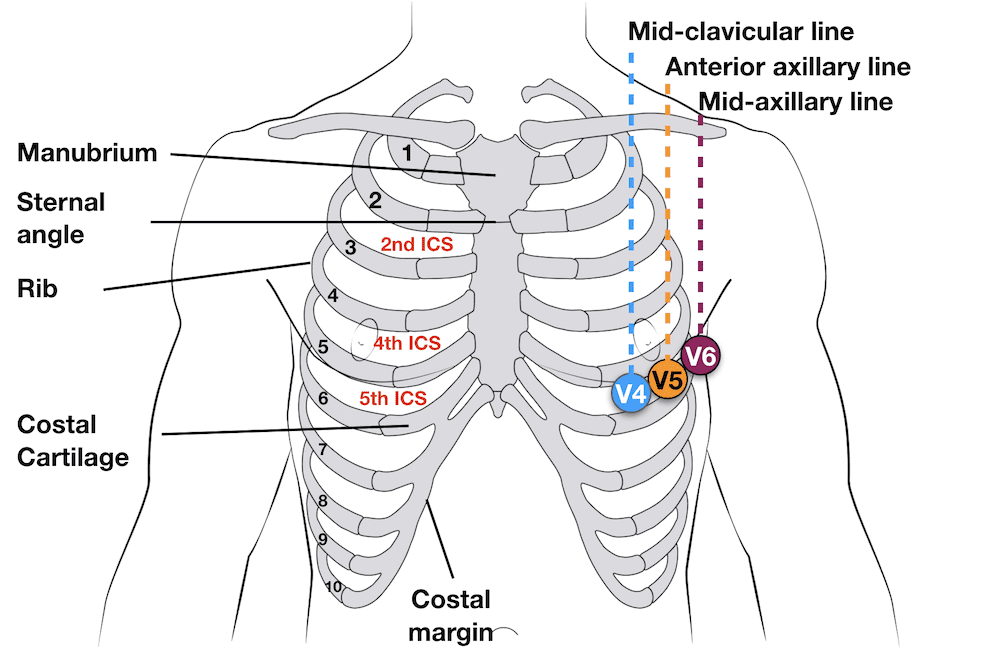
•V4 Fifth intercostal space mid-clavicular line. (Not under nipple, remember ribs curve around the chest)
•V5 – Left anterior axillary line at same horizontal plane as V4- ( lay the arm straight down the side, the electrode goes in the crease in a line with V4)
•V6-mid-axillary line in a horizontal plane alongside
•V1- 4thintercostal space at right sternal edge
•V2 – 4thintercostal space left sternal edge (not always dead opposite V1)
•V3 – midway diagonally between V2 & V4
•V4 Fifth intercostal space mid-clavicular line. (Not under nipple, remember ribs curve around the chest)
•V5 – Left anterior axillary line at same horizontal plane as V4- ( lay the arm straight down the side, the electrode goes in the crease in a line with V4)
•V6-mid-axillary line in a horizontal plane with V5 (line form the middle V5
A normal ECG should show the following:
•Positive in lead 1
•Negative in aVR
•Increase in R wave progression V1- V5 (V6 can be a little smaller)
•1 P wave for each QRS
•Normal morphologies
•Normal intervals
( note: Precordial (Chest ) leads - Variations in precordial lead placement DIAGNOSTICALLY affects the ECG, Studies have shown V1& V2 are consistently placed TOO HIGH Correct anatomical positions should be used. Deviations must be annotated on ECG)
Example of a normal 12 lead ECG

Useful reading / guidelines
Crawford J & Doherty L ; Practical Aspects of ECG Recording: M&K publishing 2012
Society of CardiologicalScience & Technology and the British Cardiovascular Society. (2010) Clinical Guidelines by consensus: Recording a standard 12-lead ECG an approved methodology.
Available at http://www.scst.org/resources/consensus_guideline_for_recording_a_12_lead_ECG_Rev_072010bpdf


